Apollo Ward (CW)https://www.chelwest.nhs.uk/your-visit/patient-leaflets/paediatrics/apollo-ward-cwhttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
We are an 8 bedded unit providing High Dependency Care to children and young people at Chelsea and Westminster Hospital.
We have dedicated staff for the unit and our team includes nurses, medical and surgical teams, pain team, play specialists and many more who will answer any questions you may have.
Who will look after me?
Each patient on Apollo Ward will have a dedicated nurse to care for them and a nurse in charge who co-ordinates the shift. The unit is led by the Unit Sister. Your dedicated nurse is responsible for looking after your child with the support of his/her colleagues throughout the shift. Nursing shift patterns run from 8am-8.30pm and 8pm-8.30am. Please ask a member of the team if you have any questions.
There is a morning ward round, consisting of consultants, registrars and senior house officers who will review the treatment and care of each patient. There is also an evening ward round.
Other members of staff
Other staff who you may meet on the ward include physiotherapists, dieticians, play specialists, ward pharmacists, housekeepers, student nurses, medical students and ward clerks.
Meals
Meals for patients are available free of charge, a member of catering staff will usually take orders in the morning.
Mothers that are breastfeeding and are visiting their child on the ward are also entitled to free meals. There is a breakfast trolley situated opposite the nurse’s base from 7.30am-10am for patients. Lunch is served at 12pm and dinner is served at 5pm.
Parent’s Room
A Parent’s Room is located on the unit; please feel free to use the room and facilities.
Car Parking
Car parking is provided to parents/guardians of patients on Apollo Ward free of charge. If you are transferred to another ward please be aware that you will have to pay for parking. Please ask your nurse for a form.
Play Team
We have a play specialist team who offer toys and games to patients as well as distraction therapy during interventions. There is also a play room located on the ward.
Televisions
The television service is available free of charge from 7am–7pm. After this time you are able to purchase a TV card from main reception for further viewing.
Please use the provided headphones from 7pm.
Visiting
There are no visiting restrictions for parents/carers. We encourage one parent to stay overnight with their child. A bed will be provided. We ask that other family members/friends visit within 8am-8pm, with no more than two visitors at one time.
School Room
The School Room is located on the 1st floor. We understand that not all patients will be well enough to attend so activities can be brought to the ward.
Art Therapy is a form of psychotherapy. It is suitable for working on a wide range of issues related to illness and hospital admission helping contain and manage some of the feelings and giving a non-judgmental space where things can be expressed.
Art therapy is a flexible, adaptable form of therapy that does not require any previous experience in art. It has been successfully accessed by many young people on the wards since 2006.
What young people and families say about Art Therapy
“Art Therapy gave him an outlet for his emotions, and we have been helped and reassured by this input. He looked forward to his sessions and the routine was settling for him. The sessions helped both our son and us and we think any child would benefit from such support.” Parent of 4 year old
“I got time to express my feelings, I really enjoyed it. I had time to focus on myself and talk to someone, draw and write what was on my mind.” 13 year old
"I like art therapy because it’s fun and gives me a chance to be messy and talk about things.” 10 year old
"It helped me with my feelings a lot, painting made me happy.” 6 year old
“Art therapy is really amazing and helps you think about your thoughts. It helps because it lets your feelings out.” 14 year old
“I think hospital admissions can be lonely and medical staff daunting. My daughter really enjoyed Art Therapy and seemed relaxed after doing it.” Parent of 8 year old
Supporting the wellbeing of young people and families
Art Therapy aims to support young people and families while in hospital.
Providing a space to communicate feelings verbally and non-verbally and offer an emotional outlet during admission.
Bell's palsy is a condition that causes temporary weakness or paralysis of the muscles on one side of the face. It is the most common cause of facial paralysis.
Other causes of facial paralysis include:
Congenital facial palsy—children born with facial weakness
Injury to the facial nerve in an accident—such as a cut to the cheek or a skull base fracture
Injury from surgery—most common during surgery of the parotid gland and neck
What are the symptoms?
The symptoms vary from person to person. The weakness on one side of the face can be described as either:
Partial, which is mild muscle weakness
Complete, which is no movement at all (paralysis)—although this is very rare
It can also affect the eyelid and mouth, making it difficult to close or open them. In rare cases, it can affect both sides of the face.
Why does it happen?
Bell's palsy is believed to occur when the nerve that controls the muscles in your face becomes compressed. The exact cause is unknown, but it is thought that the facial nerve becomes inflamed, possibly due to a viral infection.
The herpes virus is thought to be the most common cause, although other viruses may also be responsible.
Who is affected?
It is a rare condition, affecting about one in 5,000 people each year. It is most common in people aged 15–60, but those outside this age group can also suffer from the condition. Men and women are equally affected.
Treatment
Around 7 out of 10 people make a complete recovery, with or without treatment.
Most people notice an improvement in their symptoms after two to three weeks, but a complete recovery can take up to nine months. Recovery time varies from person to person and depends on the extent of nerve damage.
Prednisolone, a type of corticosteroid, is used to reduce swelling of the facial nerve.
Eye drops may be necessary if you are unable to close your eye, and tape may be used to close the eye while sleeping.
Complications
Around 3 in 10 people continue to experience weakness in their facial muscles, and 2 in 10 are left with more serious long-term problems. Complications can include:
Persistent facial weakness
Eye problems
Difficulty with speech, eating and drinking
Reduced sense of taste
Facial muscle twitching
Up to 1 in 7 people may experience a reoccurrence, especially if there is a family history of the condition.
Central line carehttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/paediatrics/central-line-carehttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
A Hickman/ central line is a thin, flexible tube which is inserted into a large vein in your child’s neck. The other end of the tube is tunnelled under your child’s skin and comes out (somewhere on the chest). This end of the line will be held in place by small stitches for as long as your child needs the line (it can be left in for weeks or months). The line will be looped and covered with a clear dressing, with small children steri strips are also used for extra security.
Please check that your child’s line is securely looped underneath the dressing. This will reduce the risk of accidental dislodgement.
You child can be sent home with a central line.
You will be provided with a safety pack containing the following items:
1 x pack sterile gauze
1 x large IV 3000 dressing
1 x small IV 3000
2 x blue clamps
2 x bionectors
4 x sani cloth CHG 2%
1 x roll transpore
The safety kit should accompany the child at all times, anyone caring for the child must be familiar with the pack and must have received safety training.
Please note that if your child develops a temperature of 38 degrees and above you should contact your local hospital immediately as your child could have a line infection or sepsis.
If worried or unsure please ring 999 and ask for an ambulance to take you to your local hospital.
Hickman/central line safety advice including daily care and observations
Infection
Observe the exit site and neck wound for any signs of infection
Redness
Swelling
Pain
Heat
Discharge i.e. blood/pus
Should any of the above occur please take your child to their local hospital or call your community nurse for assessment.
If infection is the case:
Your child will require an assessment, swabs and blood specimens to be taken
If the central line is infected then it will need prompt treatment
If the dressing is soiled with blood or there is wetness under the dressing it will need to be changed as this increases the risk of infection
If the dressing remains intact and there is no oozing then the dressing needs to be changed once a week by the children’s’ community team.
Keeping the Hickman/central line dry
The end of the central line can be taped out of the way when your child has a bath, please ensure that the end does not get submerged in the bath. Some families find it useful to place the bung in a plastic bag, using cling film or a sandwich bag and also tap the line(s) over the shoulders during bath time.
The end should not be dangling down by the nappy/groin area, if they do get soiled, the bionector (caps) at the end of the line will need to be changed and the line should be cleaned thoroughly.
If the bionector (caps) falls off, you must wash your hands thoroughly, clean the end of the cental line using a sani cloth CHG 2% for 30 seconds, allow to dry for 30 seconds and replace the bionector, ensuring that you do not touch the key parts (end of central line and the connection of the bionector. Never put the old bionector back on.
Accidental removal
If the line is removed, pressure needs to be applied immediately for 10 minutes. Using the sterile gauze in your safety pack, apply pressure to the scar on their neck and where the line came out of the chest. This is to stop any bleeding.
Please call 999 as this is classed as an emergency.
Breakage
There are two blue clamps in the safety pack that you should carry with you at all times. If the central line breaks, is accidentally cut or there is a hole in it you should;
Wrap a piece of occlusive dressing (e.g IV 3000) around the break, to ensure the line does not get dirty
Then wrap a piece of gauze around it to make the clamps fit more securely this also prevents damage that the clamps can do to the central line.
Use the two clamps provided to clamp one must above the cut/break and one closer to the chest.
Please take your child to your local hospital who will check that the central line has been clamped properly and will make arrangements to repair the line. Call an ambulance if unsure.
If you do not have the clamps with you, you should bend the line over and hold with your fingers and ring for an ambulance.
Daily checks
Check that your child’s line is securely looped underneath the dressing. This will reduce the risk of accidental dislodgement.
Check that the white clamp(s) are closed always at the thick partof the line. This will reduce the risk of blood loss if the caps were to fall off or the line broke near the hub. If you find that the clamps are open, you should close them and ask the community nurse to come and flush the line, to prevent it getting blocked.
Clavicle Fractures in Childrenhttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/paediatrics/clavicle-fractures-in-childrenhttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
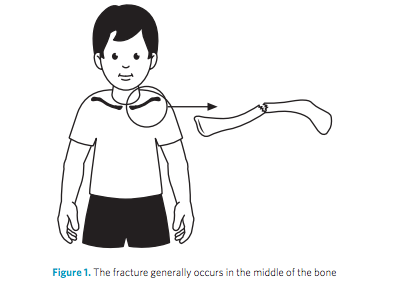
A fractured clavicle is a break in the collar bone. This is a very common fracture in children.
What are the common causes of a fractured clavicle?
It commonly happens after a falling onto an outstretched arm but can also occur after a direct blow to the chest or shoulder or from falling on to the shoulder.
What are the symptoms?
Your child may complain of pain in the shoulder/chest region. They may have an obvious bump over the collar bone.
Their shoulder may look more raised on the injured side compared to their shoulder on the opposite side. Younger children may be reluctant to use their arm.
How is it diagnosed?
The story of how it occurred and an examination of your child’s arm will help us diagnose a fractured clavicle.
An X-ray of the clavicle is performed so we will be able to see where the bone is broken and if there it is a more serious injury.
How is it treated?
This type of fracture heals well. The only treatments that are generally required are pain killers and a sling. If your child seems to be in pain they should be given simple painkillers such as paracetamol or ibuprofen.
Once the examination and x-ray have been carried out most children will be placed in a sling. Rarely does this type of fracture require an operation.
We would expect the collar bone to be painful for 4-6 weeks and your child may find it more comfortable to sleep sitting upright for a few days after the injury.
The shoulder and arm can be moved out of the sling as comfort allows. This will usually be about 2 weeks after the injury but can be sooner if comfortable.
The ‘bump’ over the fracture is quite normal and is produced by healing bone. It may take up to one year to disappear. If your child is older than ten years a small bump may remain.
Your child may return to activities as soon as comfortable, but should avoid swimming and contact sports (such as football, rugby and basketball) for six weeks.
Are there any possible complications?
There is generally an excellent return to normal function after a clavicle fracture. It is extremely rare to develop complications from a clavicle fractures.
If you are still experiencing significant symptoms after two to three months, please contact your GP or us for further advice.
Conjunctivitis is a common condition that causes redness and inflammation of the thin layer of tissue that covers the front of the eye (the conjunctiva).
People often refer to conjunctivitis as red eye.
Other symptoms of conjunctivitis include itchiness and watering of the eyes, and sometimes a sticky coating on the eyelashes (if it's caused by an allergy).
Conjunctivitis can affect one eye at first, but usually affects both eyes after a few hours.
What causes conjunctivitis?
The conjunctiva can become inflamed as result of:
A bacterial or viral infection - this is known as infective conjunctivitis
An allergic reaction to a substance such as pollen or dust mites - this is known as allergic conjunctivitis
The eye coming into contact with substances that can irritate the conjunctiva, such as chlorinated water or shampoo, or a loose eyelash rubbing against the eye - this is known as irritant conjunctivitis
Treating conjunctivitis
Conjunctivitis often doesn't require treatment as the symptoms usually clear up within a couple of weeks. If treatment is necessary, the type of treatment will depend on the cause. In severe cases, antibiotic eye drops can be used to clear the infection.
Irritant conjunctivitis will clear up as soon as whatever is causing it is removed.
Allergic conjunctivitis can usually be treated with anti-allergy medications such as antihistamines. If possible, avoid the substance that triggered the allergy.
It's best not to wear contact lenses until the symptoms have cleared up. Any sticky or crusty coating on the eyelids or lashes can be cleansed with cotton wool and water.
Washing your hands regularly and avoiding sharing pillows or towels will help prevent it spreading.
See your GP immediately if you have:
Eye pain
Sensitivity to light (photophobia)
Disturbed vision
Intense redness in one or both of your eyes
A newborn baby with conjunctivitis
School
Public Health England advises that you do not need to stay away from school if your child has conjunctivitis, unless you are feeling particularly unwell.
If there are a number of cases of conjunctivitis at one school or nursery, you may be advised to keep your child away from the school until their infection has cleared up.
Complications
Conjunctivitis can be a frustrating condition - especially allergic conjunctivitis - but in most cases it doesn't pose a serious threat to health.
Complications of conjunctivitis are rare but when they do occur they can be serious and include:
A severe case of allergic conjunctivitis can lead to scarring in the eye
In cases of infective conjunctivitis, the infection can spread to other areas of the body, triggering more serious secondary infections such as meningitis (an infection of the outer layer of the brain).
All babies regurgitate/posset/ vomit small amounts of milk after feeding. This is because food (from the stomach) comes up through the oesophagus (gullet) into the mouth. GOR happens because the muscles at the lower end of the oesophagus are too relaxed and allow milk to come back into the oesophagus from the stomach. About 40% (4 out of 10) of babies have Gastro-Oesophageal Reflux.
The doctors may diagnose this condition if:
Vomiting is particularly frequent
The child becomes particularly distressed during or after feeds or when vomiting.
Your baby is not gaining weight.
It is important to realise that GOR is not a disease. Although it is messy and upsetting, it is quite normal as your baby grows older, the muscle should open only when he or she swallows, and remain tightly closed at all other times to prevent stomach contents escaping. This is why most babies grow out of reflux by 18 months.
GOR does not mean that your child is sick. Most children grow out of it as their oesophagus and stomach develop.
What can I do to help my child?
There are steps you can take to prevent GOR.
Wind your baby regularly during feeds.
Do not over-feed your baby (ask your health visitor if you are unsure how much to feed)
If your baby is bottle fed, feed them upright and try using a smaller teat so that your baby gets their milk more slowly.
Hold your baby upright for a period after feeding.
Despite all your best efforts, some babies will continue to vomit. This is not a cause for alarm.
When should I see my GP?
If reflux happens often, or your baby is violently sick, appears to be in pain or you’re worried for any other reason, talk to your health visitor or GP – especially if they have any of the following symptoms:
Coughing, gagging or trouble swallowing
Frequent projectile vomiting
Persistent crying and being irritable
Wheezing
Bad breath
Difficulty sleeping
Arching their back during or after a feed
Drawing their legs up to their tummy after feeding
Refusing a feed even though they're happy to suck on a dummy or similar
Not gaining much weight, or losing weight.
An allergy
If you think your baby is having a reaction to infant formula or cows' milk, tell your GP. Some of the signs are a skin rash, vomiting and diarrhoea.
Your GP can prescribe special formula feeds called "extensively hydrolysed protein feeds" (see When should I see my GP?).
If your baby is allergic to cows' milk, eliminating it from their diet for two to three weeks should reduce their vomiting considerably. If you breastfeed, you'll need to exclude cows' milk from your own diet.
Some infant formula is labelled as hypoallergenic, but this is not suitable for babies with a diagnosed cows' milk allergy.
Always talk to your GP before using hypoallergenic or soya-based infant formula, as babies who are allergic to cow's milk may also be allergic to soya.
If your baby continues to vomit despite cutting out cows' milk, it's unlikely that an allergy is the problem.
Does my baby need any tests?
Usually, the doctor is able to diagnose GOR from the information you give. If the doctor is in any doubt about the diagnosis, they may recommend tests, but this is not usually necessary.
If your baby is diagnosed with GOR, your health visitor will make sure that they are gaining weight at their routine checks. If they have any concerns, they will tell you. It is not usually necessary for you to keep coming back to hospital for follow-up appointments, unless your health visitor or GP are concerned.
Are there any long term complications?
Most children with GOR grow out of it within the first six months, and it is unusual for them to still have problems after their first birthday. As long as your child is gaining weight, it is extremely unlikely that they will come to any harm from GOR.
Where can I get more information?
Your health visitor will be able to give you support, and answer your questions.
Henoch-Schonlein purpura causes blood vessels to become inflamed (swollen and irritated) the blood vessels involved are usually the small ones in the skin causing a rash that looks a bit like bruises. This type of rash is called purpura.
Other blood vessels that may be involved are the ones in the kidney, causing blood in the urine, and the ones in the intestines, causing stomach pains.
Why does it happen?
The cause of HSP is unknown. Sometimes infections, like colds, can trigger HSP. Other possible triggers are insect bites, medicines and vaccinations. It usually affects children between 2-10 years of age but it can happen to anyone. HSP is not contagious and there is no way to prevent it.
Which are the signs and symptoms?
Skin rash: This looks like small bruises or small reddish-purple spots. It is usually on the buttocks, on the legs and around the elbows. The skin rash may look very dramatic but is not dangerous.
Swelling: In many children with HSP the skin over hands and feet becomes swollen and tender. In boys this can also involve the scrotum.
Inflamed joints: Joints, most commonly knees and ankles, can become swollen and tender.
Blood in the urine: This can sometimes be seen with the naked eye (macroscopic) and sometimes only discovered when the urine is analysed with a dipstick (microscopic).
Serious kidney problems can occur but are fortunately rare.
Stomach pain: This is common and can sometimes be severe. In rare cases an abnormal folding of the bowel can occur, blocking the bowel. This is an emergency that may need surgery.
What is the treatment?
There is no specific treatment for HSP. Medicines are used only help your child feel more comfortable.
Fortunately almost all children with HSP get better without any treatment.
Painkillers like paracetamol/calpol or ibuprofen can help with joint pain. If stomach or joint pain is severe a drug called prednisolone can be used. Prednisolone may also be used along with other medicines if there are any signs of kidney damage.
About 1 in 3 children who have had HSP will get it once again in the first 6 months.
What follow up will be needed?
Your doctor will want to check urine samples and blood pressure several times to check for kidney problems. These checks should go on for at least 6 months. Your child should receive an appointment in the Paediatric Outpatient Clinic within 1 month from when the HSP started. Your GP may also carry out some of these checks and may prescribe you urine dipsticks that can be used at home.
The long-term follow-up for urine and blood pressure checks are very important.
When to come back to A&E?
If your child gets increasing stomach pains, vomits, blood in the stool (poo) or in the urine, worsening swelling or pains bring them back to the A&E department.
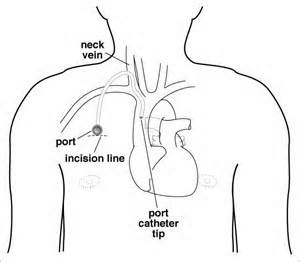
The port is especially susceptible to infection during the first two weeks after an operation.
Keep both incisions (on the neck and by the port) dry for the first week after the operation. After one week your child may have a bath, and if steri-strips are still present they can be removed.
Observe the incisions, by the port and on the neck for signs of infection:
Redness
Swelling
Discharge ie blood or pus, from either incision
Pain
An infection of the skin over the port needs to be treated promptly as it may progress to a line infection. Contact your local hospital / paediatric community nurse if there are any signs of infection.
Do not go swimming when the port is accessed
Always check the port daily for signs of infection
The most important part of caring for a child with a very low neutrophil count is prompt investigation and treatment if they become unwell or develop a fever. For immunosuppressed children- if your child seems unwell and feels hot whilst neutropenic, take their temperature. One possible cause of a temperature is an infection inside the port.
If their temperature is raised to 38.5°C once, or is 38.0°C for one hour, phone the doctor at your local hospital. Your child will need to be admitted to hospital, so you need to take them there promptly, for examination, and to have blood cultures taken. A course of intravenous antibiotics will be commenced.
Ensure you are given some Ametop gel (anaesthetic gel) to take home with you.
If you have a community nurse you may need some supplies to take home with you. We will check with your local that they have some needles, if they don't, we will give you some to take with you.
When someone is removing the needle the port will need supporting so as not to pull the port away from the muscle that it is sutured to.
We are a dedicated 12 bed unit for young people and adolescents aged 11–16 years, at Chelsea and Westminster Hospital. We take admissions from A&E and transfers from other hospitals.
Nursing and support workers
Jupiter has a team of nurses and healthcare assistants who will look after your child, led by the Ward Sister. Day shifts are 8am–8:30pm and night shifts 8pm–8:30am.
Boys and girls are different!
For this reason we have separate areas for boys and girls to sleep in. We also have separate bathrooms, and a shower room. On occasion, we may have to change the bays around if we have too many boys or girls.
The lights are switched on at 8am and your child’s nurse will come round to wake them up. At night we expect all of our patients to be in bed no later than 10pm. The main lights will be switched off between 9–10pm. Patients may leave their bedside light on.
Meals
Breakfast is served from a trolley outside the kitchen. Patients can help themselves to toast and cereal. Their nurse will be able to help them with meals if needed.
Lunch and supper is chosen from a menu that will be brought round each morning. If you do wish to bring in any of your own food, then ask the nurse for a label and it may be placed in the fridge in the parents’ room.
Breakfast: 7:30–9am
Lunch: 12 noon–1pm
Dinner:5–6pm
Water jugs are filled and refreshed twice a day. There is also a water fountain and squash on the ward. The nurse will let you and your child know if they are not allowed to eat or drink.
School
If children are well enough, we expect all young people to attend the hospital school, which is on the first floor. If they cannot attend then the teachers can bring work to the bed side. If a child is with us for a while, the school will liaise with their own school for work to be brought in for them.
Please note that we inform school nurses of all admissions to hospital.
School times: Mon–Fri, 10am–12 noon and 1:30–3:30pm
Parents/carers
The ward tries to promote independence with young people, and for this reason we do not encourage parents to be resident overnight. As a ward, we are provided with limited parents beds but we do have use of the patient hotel should you wish to stay.
There is a parent’s room on the ward, with tea and coffee facilities. If you put anything in the fridge, please ensure it is labelled; otherwise it may be thrown away.
Visitors
Please, no more than two visitors at a time. Parents may visit any time between 8am–10pm.
As we expect all children to be in school, we do not encourage other visitors until after 3:30pm, especially if school friends are coming to visit. Any visitor under the age of 16 years MUST be accompanied by an adult at all times, otherwise they will not be allowed on the ward. All other visitors must leave by 8pm.
TV/phone
The television service is available free of charge from 7am–7pm. After this time, you are able to purchase a TV card from the main reception for further viewing.
We ask patients to respect their fellow patients on the ward so if they are watching TV or listening to music we encourage them to ask for some headphones.
If you or your child has a mobile phone, please have it on silent while on the ward.
Youth worker
We have a dedicated youth worker for the ward who works three days a week on Mondays, Wednesdays, Fridays and occasional Saturdays. The role of the youth worker is to provide age appropriate activities and support adolescents emotionally during their time in the hospital by building positive relationships with them. We also have a common room for Jupiter patients to use should they wish to play games or just have some time away from their bed space.
Youth forum
The youth forum called HYPE (Hospital Young People’s Executive) gives former and current patients aged between 12 to 17 an opportunity to meet every 6 to 8 weeks to have their say on the services they receive. Young people can also share their hospital experiences to help the staff understand what young people want and need.
The Youth Forum have undertaken various projects so far, such as taking an in house tours of the catering department in order to change the adolescents food menu, going on local trips, designing posters, and much more.
Going home
Medicines
If your child requires medication to take home your doctor will prescribed it and the pharmacy team will arrange for it to arrive to the ward. At times this process can take a few hours to safely arrange, therefore please be patient and bear in mind your nurse will be following up the progress on this on your behalf.
Car parking
We provide reduced car parking rates for parents of children who are inpatients to £10 for 24 hours. Please ask your nurse for a voucher.
Kawasaki disease is a rare condition that mainly affects children under the age of five. It is also known as mucocutaneous lymph node syndrome. The characteristic symptoms are a high temperature that lasts for more than five days, with:
Rash
Swollen glands in the neck
Dry, cracked lips
Red fingers or toes
Red eyes
By weeks 2–4, symptoms will become less severe but may last longer. At this stage, the affected child may have peeling skin on their fingers and toes.
See your GP if your child is unwell with the above symptoms. The symptoms of Kawasaki disease can be similar to those of other conditions that cause a fever in children.
Kawasaki disease cannot be prevented but if it is diagnosed and treated promptly, most children will make a full recovery within six to eight weeks.
It is thought that Kawasaki disease is caused by an infection, although the exact cause is not clear.
Treating Kawasaki disease
Kawasaki disease is usually treated in hospital because it can sometimes lead to serious complications
It is best if treatment begins as soon as possible, ideally within 10 days of the symptoms starting. The sooner treatment starts, the quicker the recovery time and the less risk there is of complications developing.
Aspirin and intravenous immunoglobulin (a solution of antibodies) are the two main medicines used to treat Kawasaki disease.
Complications of Kawasaki disease
Kawasaki disease causes the blood vessels to become inflamed and swollen, which can lead to complications in the coronary arteries (the blood vessels that supply blood to the heart).
Up to 5% of children with Kawasaki disease experience complications with their heart. In about 1% of cases, the complications can be fatal.
Because of this, the condition has become the leading cause of acquired heart disease (when the heart's blood supply is blocked or interrupted) in the UK.
Who is affected?
In the UK around eight in every 100,000 children develop Kawasaki disease each year.
Research carried out in England from 1998 to 2003 found that 72% of children with Kawasaki disease were under five years old. The condition was also shown to be one-and-a-half times more common in boys than in girls.
A lumbar puncture, also known as a LP or spinal tap, is a test where a doctor uses needle to collect fluid from your child’s lower back. This fluid is called cerebrospinal fluid, or CSF, which surrounds the brain and spinal cord. A small amount of CSF is collected and sent to the laboratory for testing.
Why does my child need a lumbar puncture?
A lumbar puncture is needed to test the fluid around the brain and spinal fluid. This is most commonly to look for infection. In this case, the test is done to find out if a child has an infection called meningitis, which is a serious infection around the brain.
It is important for your child to have the lumbar puncture as it is the only way to know for sure if they have meningitis. Early diagnosis of meningitis can greatly improve long term outcomes. Having a lumbar puncture doesn’t necessarily mean that your child has meningitis but is an important test to rule this serious infection out.
A lumbar puncture may sometimes be carried out to look to for rarer conditions, often involving the neurology team.
How is a lumbar puncture carried out?
Younger children will be placed on their side with their knees tucked into their chest or curled up into a ball and will be held in this position by an assistant. Older children may be asked to sit on the edge of the bed, leaning forward hugging a pillow.
The back is carefully cleaned and the surrounding parts of the back draped with a sterile gown. The doctor puts a needle into the spaces between the vertebrae (bones of the spine) below the level of the spinal cord. The fluid will be collected into special containers and will be sent to the laboratory for testing.
The whole procedure may take up to 45 minutes, although much of this is preparation time. We generally advise parents to step outside during the procedure.
Does it hurt?
It is an uncomfortable and sometimes painful test. Your child will be held still, and babies and small children do not like this and will often cry.
Depending on the age of your child we can help to numb the skin with some cream, or with an injection, or we may be able to give your child some medicine to make them feel calmer and less scared.
Is it dangerous?
A lumbar puncture is a very safe test and it is unusual for something to go wrong. Sometimes we are not able to get fluid and may have to try more than once. A small number of children may have headache or backache for a day or two after the test. The risk of any serious complications, including bleeding, infection or damage to nerves is extremely small.
It understandable to feel uneasy or anxious but it is important to know that a lumbar puncture is a very safe and common test, and complications are rare.
Care after the procedure
A plaster or dressing will be placed on your child’s back which can be taken off the next day or left to fall off by itself. If they have a headache or backache painkillers can be given. Your child will be encouraged to lie flat for about an hour afterwards. When he or she is fully awake, you should encourage him or her to drink normally.
Getting the results
The fluid is sent to the laboratory for testing.
If the lumbar puncture was carried out to look for infection then some results will be available within 4-6 hours while others, including trying to identify the specific bacteria, will usually take 48 hours, and sometimes up to 5 days.
If the lumbar puncture was carried out for any other reason it is likely that some results will be available in 4-6 hours, but the most important tests may take days, or in some cases weeks. The team performing the test should be able to advise you when to expect to hear the results.
The doctors will give you the results when they become available.
The main function of the kidneys is to clean blood by filtering out excess water, salt and waste products from food. However when the kidneys have damaged filters protein can leak into the urine. As a result there is not enough protein in the blood to soak up the water and therefore the water moves into the body tissues causing swelling and a greater chance of catching infections.
It can affect people of any age, but is often first seen in children aged between two and five years.
Children with nephrotic syndrome have times when their symptoms are under control (remission), followed by times when symptoms return (relapses). Most will relapse less frequently as they get older, eventually "growing out of it" by their late teens.
Symptoms can usually be controlled by medication. Most children with nephrotic syndrome respond well to steroids and aren't at risk of kidney failure.
However, a small number of children have congenital (inherited) nephrotic syndrome and usually do less well.
What problems can it cause?
Some of the main symptoms associated with nephrotic syndrome are:
Swelling
The low level of protein in the blood reduces the movement of water from surrounding tissues back into the blood vessels, leading to swelling (oedema). Swelling is usually first noticed around the eyes, then around the lower legs and rest of the body.
Infections
Antibodies are a specialised group of proteins in the blood that help fight infection. When these are lost, children are much more likely to get infections and frequently experience fatigue, poor appetite and weakness.
Urine changes
Occasionally, the high levels of protein being passed into the urine can cause it to become "frothy". Some children with nephrotic syndrome may also pass less urine than usual during relapses.
Blood clots
Important proteins that help prevent the blood from clotting can be passed out in the urine of children with nephrotic syndrome. This can increase their risk of potentially serious blood clots.
Diagnosis
Diagnosis is made with a simple urine test and blood test. In very few cases a kidney biopsy is required.
Symptoms:
High levels of protein in urine.
Low levels of protein in the blood.
Less frequent urination.
Weight gain from excess water.
Oedema (swelling) resulting from build-up of salt and water.
Vomiting and diarrhoea due to abdomen swelling.
Skin breakdown during periods of oedema – very pale skin.
Managing nephrotic syndrome
The main treatment for nephrotic syndrome is steroids, but additional treatments may also be used if a child develops significant side effects.
Steroids
When they are first diagnosed, your child will normally be prescribed at least a four week course of the steroid medicine prednisolone. This will need to be taken every day, followed by another four weeks where the medication is taken every other day. This stops protein leaking from your child's kidneys into their urine.
When prednisolone is prescribed for short periods, there are usually no serious or long-lasting side effects, although some children may experience increased appetite, weight gain, swollen cheeks and mood changes.
Most children respond well to treatment with prednisolone, with the protein often disappearing from their urine and the swelling going down within a few weeks. This period is known as remission.
Diuretics
Diuretics, or "water tablets", may also be given to help reduce the fluid build-up. They work by increasing the amount of urine produced.
Penicillin
Penicillin is an antibiotic and may be prescribed during relapses to reduce the chances of an infection.
Dietary changes
To prevent further water retention and oedema, you may be advised to reduce the amount of salt in your child's diet. This means avoiding processed foods and not adding salt to what you eat.
Vaccinations
Children with nephrotic syndrome are advised to have the pneumococcal vaccine. Some children may also be recommended the varicella (chickenpox) vaccination between relapses.
Live vaccines (such as MMR, chickenpox and BCG) should not be given while your child is taking medication to control their symptoms.
Caring for your child at home
If your child has been diagnosed with nephrotic syndrome, you will need to monitor their condition on a daily basis to check for signs of relapses.
You will need to use a dipstick to test your child's urine for protein the first time they urinate each day. The result for each day will need to be written down in a diary for your doctor to review during your outpatient appointments.
You should also note down the dose of any medication they are taking and any other comments, such as whether your child is feeling unwell.
If the dipstick shows +++ or more of protein in the urine for three days in a row, this means your child is having a relapse. If this happens, you either need to follow the advice given about starting steroids or contact your doctor.
You should seek immediate medical advice if:
Your child has come into contact with someone who has chickenpox or measles
Your child is puffy, unwell or has a fever
Your child has diarrhoea and is vomiting
Support
There is help and support available from various medical professionals involved in your child’s care and treatment.
Neptune Ward is a 16-bed medical ward at Chelsea and Westminster Hospital. We take admissions from A&E, outpatients and transfers from other hospitals.
We are also a shared care ward for children receiving oncology treatment. We care for children and from birth to 16 years of age. We have a large team of nurses, doctors and specialists who are committed to providing a high standard of care to your child, working in partnership with families and carers.
Nursing and support workers
Neptune Ward has a team of nursing staff and health care assistants who will look after your child, led by the ward sister.
Day shifts are 8am–8.30pm and night shifts are 8pm–8.30am. Other members of our team also include play specialists, domestics and administrative staff.
Medical
Your child’s care will be led by a consultant who has a team of doctors working with them. You will be seen by a member of the medical team on admission and by a consultant within 24 hours of your child’s admission to the ward.
A consultant-led medical ward round is carried out daily from 9am–12pm. Other specialist teams may visit at different times.
Visiting times
Visiting times are 8am–8pm, parents can visit outside these times.
We do have limited space and in order to be respectful of other patients we can only have two visitors per bedside at one time. If you are allocated to a side room this will be for a medical reason and visiting may need to be restricted. Please ask your child’s nurse if you are unsure.
Staying overnight
We recognise the importance of family-centred care and strive to achieve a safe and comforting environment for the child. We therefore welcome one parent or guardian to stay alongside your child overnight and when possible we will provide a camp bed. We do ask that these are folded away in the morning by 9:30am in order to keep a clean, tidy and safe bed space.
Overnight we would like the children to have as good a night’s sleep as possible to aid their recovery. We will therefore endeavour to keep noise to a minimum, however sometimes monitoring and machinery is necessary. Bedside lamps or dimmed overhead lights will need to remain on in order to ensure your child can be assessed at all times to maintain their safety.
Parents room
This is for parents only. Please use this room as a children-free zone away from the patient bedside to allow yourselves a bit of space.
Please feel free to bring in your own food items or home cooking and make the most of the facilities. We ask that the area remains as clean and tidy as when you found it, ready for the next parent. Please label all food in the fridge with your child’s name and the date in order to maintain a safe food environment—food will discard if unlabelled.
Mealtimes
Breakfast is served from a trolley outside the kitchen. You can help yourself to toast and cereal. Your nurse will be able to help you if needed.
Lunch and supper is chosen from a menu that will be brought round to you each morning, for you to make your own selection.
Breakfast: 7:30–9am
Lunch:12 noon–1pm
Dinner:5–6pm
Water jugs are filled and refreshed twice a day. There is also a water fountain and squash available on the ward.
Playroom
We have a playroom which is open from 9am. It is a safe area for children to explore and play. We have play specialists and play assistants who can provide distraction techniques during procedures, play interaction and support, and one-to-one play with your child. All children and siblings must be supervised at all times when in the play room.
School
If well enough, we expect all young children and adolescents to attend the hospital school. It is located on the 1st Floor of the hospital. If your child cannot attend the school, teachers can bring work to your bedside.
If your child is in hospital for a while, the school will liaise with his/her own school for work to be brought in.
Please note that we inform school nurses of all admissions to hospital.
School times are (Monday to Friday): 10am–12pm and 1:30–3:30pm.
Televisions
The television service is available free of charge from 7am–7pm. After this time you are able to purchase a TV card from the main reception for further viewing.
We encourage headphones to be worn whenever possible in order to be respectful of noise to those around you.
Going home medicines
If your child requires any medication to have at home your doctor will prescribe it and the pharmacy team will arrange for it to arrive on Neptune Ward.
At times this process can take a few hours to safely arrange, therefore please be patient. Your nurse will keep you up-to-date with any progress.
Car parking
We provide reduced car parking rates for parents of children who are inpatients (£10 for 24 hours). Please ask your nurse for a voucher which you can hand in at main reception with your car park ticket when you leave.
Feedback
We welcome all feedback and encourage you to complete the children’s feedback survey available at the ward desk. Please ask your nurse or the receptionist for the form
Paediatric Assessment Unit (PAU)https://www.chelwest.nhs.uk/your-visit/patient-leaflets/paediatrics/paediatric-assessment-unit-pauhttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
The PAU is an emergency assessment unit for children and young people where they can referred by their GP, Midwife, Health Visitor, Urgent Care Centre (UCC) and/or the Paediatric Emergency Department (PED).
The Unit provides a rapid assessment of children and young people and aims where clinically possible to assess, treat and discharge home in a short space of time. Children and young people are admitted under the care of a consultant paediatrician who will ensure that the appropriate assessment and care is given.
What to expect during your visit
The nursing staff on PAU aim to complete an initial assessment of your child or young person within 15 minutes of arrival to the unit. At times this may not be possible if for example a lot of people have arrived in a short space of time.
If you are worried your child has deteriorated please inform the nurse.
On assessment you will be asked lots of questions to ensure you are seen in a reasonable amount of time. This often means you are not seen in the order you arrives as other children may need to be seen before you if their condition is more serious.
You will be seen by a member of the medical team usually within one hour of arrival. At this point any tests, investigations or treatment will be started.
The results of most tests we carry out will be available within a few hours and will help the medical and nursing staff make decisions with you about what care is needed.
You will also require a period of observation before being discharged home. The PAU is not an inpatient ward, although sometimes children will stay overnight for a longer period of assessment. The PAU is a busy environment. For this reason we ask that you supervise your child at all times, especially in the play and waiting area.
If we feel you will not be able to be assessed and treated quickly or you do not respond to initial treatment then you may need to be admitted to a Paediatric Ward for ongoing care.
Going home from PAU
The PAU is open 24 hours a day, 7 days a week, and treats a large number of children. Therefore it is essential once your treatment is complete you are able to leave the department and continue the care of your child or young person at home.
If you are unable to arrange your own transport home, please ensure that the staff are aware of this as early as possible to allow us time to assist your with this if required.
Once you leave the PAU you will be given a discharge information leaflet. This will have a brief summary of your visit including why you attended, what treatment has been given and any further advice or treatment we would like you to continue at home.
The discharge leaflet also gives advice on what to look out for in your child once at home including any signs that your child is becoming more unwell.
Some children will need to be seen again by the paediatric team following discharge. For this purpose you may be asked to see your GP or receive and appointment to see a paediatrician in our Rapid Access Clinic (RAC).
Some children and young people will be asked to attend the PAU or RAC for on-going treatment such as dressings or the administration of medications.
All children and young people who attend our hospital automatically have a referral made to their Health Visitor or School Nurse and their GP. This information is usually made available for them within 48 hours of your visit.
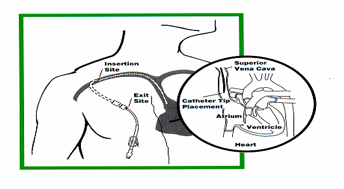
PICC stands for “Peripherally Inserted Central Catheter”. It is a silicone rubber tube, which is placed in the antecubital fossa of the arm (the elbow crease) with the tip of the catheter lying in the superior vena cava, the large vein at the entrance to the right atrium of the heart. It is held in place by two small stitches in the skin. Their use appears to be associated with a lower rate of infection.
This may be due to the fact that the antecubital fossa is less colonised with normal skin “bugs” and is less oily and moist than the chest and neck.
For smaller children or babies the same line is used but will be placed on the chest, this is called an uncuffed skin tunneled central venous catheter. It is tunneled under the skin of the chest wall to a vein in the neck. From there it is threaded through a large vein into the right atrium of the heart.
The PICC can stay in position for many months without causing any problems.There is a special tip at the end of the catheter called a Groshong™ valve.
This is a 3-position, pressure sensitive valve. It allows fluid infusion and blood aspiration. When the PICC is not in use, the valve maintains catheter patency by restricting the backflow of blood and preventing air embolism by remaining closed. This means there is no need to use clamps and heparin between each use of the line.
What care does the catheter require?
The catheter is looked after aseptically which involves careful hand washing, wearing gloves and being very clean. You will also notice a cap on the end of the catheter to protect the end.
When not in use, the PICC line has to be flushed once a week with a saline solution.
The exit site dressing also needs to be changed once a week. The old dressing is removed and the skin is cleaned with an antiseptic solution. A small loop is placed in the line and steri-strips help to secure it. A clean dressing is then reapplied. If the dressing becomes loose, wet or dirty, it must be changed immediately.
Safety aspects For PICCs infection
Observe the exit site (where the tube comes out of the arm) for any signs of infection:
Redness
Swelling
Pain
Discharge ie blood or pus
If this should occur take your child to your local hospital or call your paediatric community nurse for assessment, swab and blood cultures. An infection needs to be treated promptly as it may progress to a line infection (infection inside the catheter).
If your child’s temperature is 38.0ºc or above go straight to your local hospital. This is because when children are feverish and unwell, they are very susceptible to infection and the PICC line is a possible source of infection.
If the dressing is soiled with blood or looks wet under the dressing, it will need changing, as this increases the risk of infection. Otherwise the dressing needs changing once a week, your community team will do this.
Try to keep the PICC - including the ends, dry. Tape it up out of the way when your child is having a bath.
If the cap falls off, wash your hands well, clean the end of the PICC with an alcowipe being careful not to touch the end, and put on a new cap. Never put back on an old cap. Please tell your community nurse so that blood cultures can be taken.
Accidental removal of line
Please ensure that the PICC is securely fastened with steri-strips and that it is completely covered to half way down the hub with IV 3000. If possible the PICC should be looped underneath the dressing to prevent accidental damage or dislodgement. When not in use the area around the PICC can be covered with a bandage to provide extra security.
If the line is accidentally removed, pressure should be applied, for 5 to 10 minutes, to the exit site, to stop any bleeding.
If the line falls out, take your child and the PICC to the ward at your local hospital.
Broken line
You will be given some blue clamps to take home with you. Ensure you carry them around with you at all times.
If the PICC breaks, or you can see a hole in it, clamp the line between the exit site and the break. The line can be mended, so wrap a piece of occlusive dressing (e.g. a small IV3000) around the break to ensure that the line doesn't get dirty. Then place a piece of gauze around the line before you apply the clamps. These prevent air getting in and blood coming out of the line.
Use the third section of the blue clamps (at the bottom of the "V"), as the first section may damage the line further, and the second section won't clamp the line sufficiently. If you don't have your blue clamps on you, bend the line over and hold it with your fingers. Take your child up to your local hospital to have them assessed and to check that the line has been clamped properly. They will make arrangements with us to have it repaired
If you do not have the clamps with you, you should bend the line over and hold with your fingers and ring for an ambulance.
Play in Hospitalhttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/paediatrics/play-in-hospitalhttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
Play is a familiar language used across the world by children as they explore, learn and understand about their world and the people in it. That language can be lost in times of illness, injury or trauma—but rarely is it needed more.
Play is recognised by the Department of Health as essential support for children coping with illness and hospital life [NSF: 2003]. It is an invaluable communication tool for all of us to use when supporting children’s specialist developmental needs. Babies, schoolchildren, young people, their families and paediatric staff can greatly benefit from a professional play service supporting them throughout a variety of healthcare experiences.
Hospital play staff
Chelsea and Westminster Hospital has a well-established Play Service which offers a range of expertise and resources for all children and families . Our team of hospital play specialists and assistants have completed professional training to use play in healthcare. They offer a variety of strategies including normalising/developmental play, emotional outlet/therapeutic play, procedural play and physiological play.
Our aims
Through play we aim to provide:
An essential degree of normality for children and their families in abnormal surroundings
Developmental play facilities in all areas of the hospital where children are cared for
A lowering of stress and anxiety for children, families and other staff
A raised understanding of the benefits of specialist play in healthcare
What we provide
Visits before admission to help children and their families become familiar with the hospital and staff
A range of developmental toys, games and play activities to help reassure babies, children and teenagers across the children’s wards and in children’s outpatient areas.
Play preparation working with parents and other staff using medical play to help children understand their hospital experiences at an appropriate level.
Teaching of distraction and relaxation techniques for families, children, teenagers and staff to help raise coping skills during treatments.
Therapeutic play sessions supporting children and teenagers as they process feelings about their hospital care and illness.
Use of our sensory play rooms offering a range of multisensory experiences.
A teaching programme for multidisciplinary teams and affiliated agencies using the practical and theoretical aspects of play within healthcare.
Referral service for children and teenagers benefiting from one-to-one support.
Play rooms and children’s wards
Monday–Friday: Play rooms on the wards are open on a supervised basis at the discretion of the play specialists (depending on the demands of the service and in line with infection control guidelines). At mealtimes the play rooms will be closed for cleaning.
Evenings and weekends: During evenings and weekends the play rooms are open at the discretion of the nursing staff. Hospital play specialists are currently not available at these times.
Children’s Outpatients
Hospital play staff are available throughout Mondays to Fridays offering a range of activities. You can also ask for individual support for a child who may be experiencing difficulties coping with examination and treatment.
We ask that you please do not leave your children, including any brothers and sisters, unattended in the waiting area without speaking with the hospital play specialist first.
Parents and carers
As a parent or carer you play an important role in helping to create a sense of normality for your child while they are in hospital.
We encourage parents and carers to stay with their children and join in with play opportunities throughout the day.
It is important that families and staff speak with their play specialist before leaving a child within the play areas. We can only offer limited supervision during parent/carer absence as we may be called away to support other children at any time
Play Service
‘Play can be a therapy, a medicine and a natural healer that promotes humour, happiness and wholeness... an absence of fun, little or no playtime and a lack of laughter are common symptoms of stress, sickness and disease.’
All the freely movable joints of the body have a lubricating lining called the synovial membrane. Irritable hip occurs when the membrane becomes inflamed for a short period of time (otherwise known as ‘transient synovitis’).
The inflammation causes pain. The synovial membrane produces more than its usual thin film of lubricating fluid when it is inflamed and this can result in more pain in the joint.
Irritable hip occurs in children (usually aged between 3 and 10 years) and is more common in boys than girls.
What causes irritable hip?
Unfortunately no one knows the cause. It may be due to a virus, or perhaps a reaction to an infection somewhere else in the body.
What problems can it cause?
The inflammation in the joint sometimes happens after a flu-like illness. A child will complain of pain in one hip on walking. The pain can be felt in the groin, thigh or even the knee on that side. You may notice that your child is walking unevenly or limping.
How is the diagnosis made?
The diagnosis is usually made from the history and description of the problem and from the examination and observation of your child.
It may be that X-rays and / or blood tests are taken, but this is not always necessary. Your doctor will want to rule out other, more serious problems that can look similar to irritable hip.
One of the most important of these is a bacterial infection in the hip, which needs to be diagnosed and treated relatively quickly to prevent any damage occurring to the hip joint.
How should it be treated?
Children with irritable hip may find walking and standing painful. They should be allowed to rest so that pain is avoided.
It may help to lie on their back and find the most comfortable position for their leg.
An anti-inflammatory medicine, such as ibuprofen may be recommended to ease the swelling of the synovial membrane. Simple pain killers such as paracetamol may also help.
Your child should not take part in sporting activity (apart from gentle swimming) for a couple of weeks after the illness.
When to come back to A&E?
You should return to A&E if:
Your child is not better after 7 days of rest
Your child develops a high temperature or is generally not well in himself or herself
Your child is in more pain or is not able to put weight on their leg to walk
In most cases you will have been given a review appointment (often in the Paediatric A&E) in two or three days’ time.
Skin care for children with eczemahttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/paediatrics/skin-care-for-children-with-eczemahttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
Emollients are designed to soothe and hydrate the skin
Ointments are better for dry skin as they form a layer on the skin
They are safe to use and the effects are short lived therefore they must be applied often but you do not need to apply thickly
If emollient is in a tub, a spoon should be used to decant some onto a saucer as this will prevent contamination of the creams
Emollients should be applied quickly and gently onto skin in a downward movement in order to minimise plugging of the hair follicles, which can lead to infection
Encourage your child to apply emollients each time you see them scratching
Regular and frequent use of the emollients can go some way to reducing a flare-up of eczema.
Bath emollients
To minimise stinging, apply a soap substitute before entering the bath
They are designed to disperse in water and coat the body on entering and leaving the bath
Water should be tepid, as hot water will cause irritation to the skin
Pat dry as rubbing will cause irritation.
Topical steroids
These are needed to control the eczema as they reduce inflammation
Only use what your doctor prescribes and never be tempted to use other people’s prescriptions
You should decant some onto a saucer and apply enough to show a fine visible film to all areas of eczema
It should be applied twice daily unless your doctor informs you otherwise
When you see an improvement, try reducing application to once daily
If control of the condition is maintained, you can try applying the topical steroid on alternate days and so on until eczema is controlled
If your child has a flare-up of eczema you should go back to twice-daily application of topical steroid, or contact your GP
Leave approximately 30 minutes between steroid and emollient application to avoid dilution of the topical steroid
Skin care should become part of your everyday routine—please do not be tempted to miss any treatments.
Hair and scalp care
Hair should be washed and rinsed separately from your bath as the shampoo may irritate the skin
If a medicated shampoo is used, massage it onto the scalp and leave for five minutes before rinsing
If eczema is on the scalp avoid use of hair dryer as the heat will cause irritation.
Infection
Staphylococcus aureus is an organism that is found on the skin of most children with eczema and can be there without causing any problems. However, sometimes when the skin is damaged through persistent scratching it may lead to infection.
Symptoms that suggest your child may have developed an infection include:
sudden deterioration in your child’s eczema
your child is unwell
eczema is wet and weeping.
Your doctor may take a skin swab to check that the correct antibiotic is prescribed.
When the skin is infected you should not use ointments but change to a cream as the ointment acts as a protective cover and will prevent oozing, which could make the eczema worse.
Streptococcus infection is another organism which can cause skin infection. Your child’s skin may be very red and they may be unwell.
It is often possible to treat these infections at home with antibiotics but remember it may be necessary to admit your child to hospital for a few days.
Herpes simplex virus (cold sores)
Children with eczema should be kept away from those with cold sores and if you have one, please avoid kissing your child.
Children with eczema have an abnormal response to this virus and it will quickly spread.
You can recognise it as clusters of little blisters grouped together or eroded lesions.
If you suspect your child has contracted cold sores, please see your GP immediately as you will need to get an antiviral medicine.
If it is widespread your child will be admitted to hospital for intravenous antiviral drugs.
Treatment notes
Avoid extremes of temperature
Use non-biological washing powder and no fabric softeners
Avoid scented products
Avoid wool garments
Damp dust and vacuum the sleeping environment daily—try to do this when your child is not around
Bedroom should be cool and well ventilated
Avoid contact with animal hair/fur
Please note: If using Pimecrolimus or Tacrolimus cream please see product box for further information.
This is a common condition of infancy and is characterised by erythema (redness) and yellow scale on the scalp and sometimes the eyebrows. Unlike atopic eczema it is not itchy, uncomfortable or painful but can look unsightly.
It generally affects infants under three months of age, occurring mainly on the scalp (as cradle cap), eyebrows, face and limb flexures. It can also affect the nappy area.
It will generally clear on its own with mild emollient therapy—for example, emollient bath once daily and application of emollient creams.
It may be necessary to use a mild topical steroid on the affected areas of skin, but your doctor will assess and advise which treatment is necessary.
Treatment
Bath once daily in a bath emollient
Apply moisturiser twice daily
Apply any medicated creams as directed by the dermatology nurse.
Cradle cap
Cradle cap varies in severity from mild covering of dry flaky skin to a thick scaly scalp. It is generally a greasy yellow scale with a tell-tale crusted appearance.
Treatment
Use a bland emollient or petroleum jelly to gently massage onto the scalp and leave for 30 minutes. Oil must not be left on the scalp as it can block hair follicles and cause subsequent infection—therefore a mild baby shampoo is recommended to wash it off.
A soft baby comb/brush or cloth can then be used to gently remove loosened scales
Do not pick at the scales as this can lead to damage of the hair follicle and result in permanent hair loss.
If scalp has an offensive odour, there may be a secondary infection.
You may be given a cream by the doctor to treat this. It should be applied after the treatment detailed above.
If you have any worries or concerns please contact your GP.