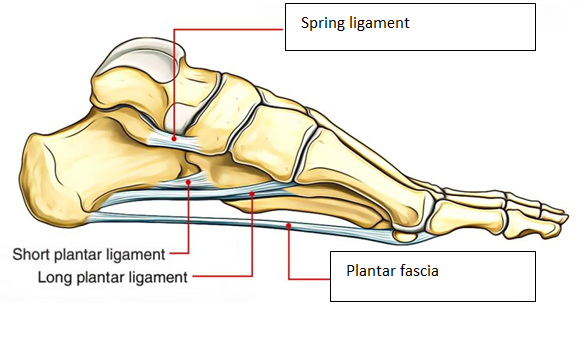
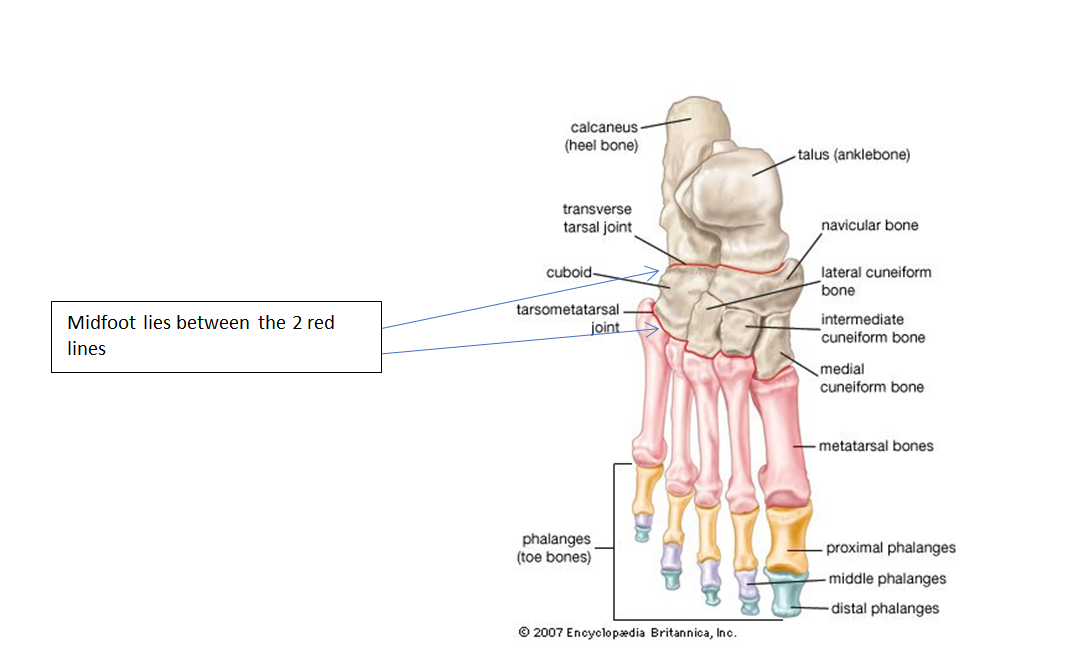
The midfoot is the apex of the arch where the metatarsals and the hindfoot joints are connected by intricately connected short bones. These small bones allow gliding movements, improving the efficiency of the foot when walking, whilst supporting the weight of the body. The position of the bones is maintained by interlocking joints along with the ligaments, muscles and fascia.
The height of the foot arch can vary from low to high and still function normally, at the extremes of these two presentations the arch would be considered abnormal, or if the arch height changed over time. The exception to this is during the development of the foot from infant to the preschool child.
Common complaints
The most common arch complaints stem from arthritis, fracture or birth abnormalities.
Midfoot arthritis can result from long term poor alignment, overuse or an injury to the supporting soft tissues (ligaments and tendons). Acute injuries occur when the force overwhelms the local structures, for instance a head on car collision, when the individual tries to brace themselves against the impact.
Spraining the foot when running or walking, here the forces going through the foot can be several times body weight. However, the chronic repetition of joints being unevenly stressed over years, is often the most common cause. The symptoms can be severe limiting walking and standing and are normally relieved by rest.
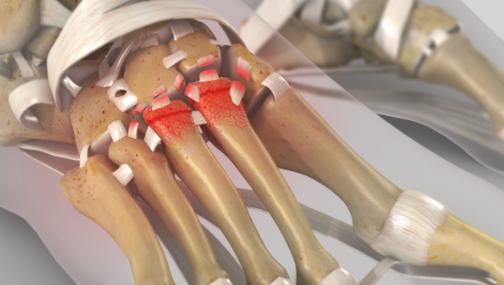
Lisfranc injury with the tearing of ligaments, fracturing of the metatarsal bases and loss of alignment.
Diagnosis
The diagnosis is made by a clinical examination of the foot and the patients’ walking pattern. The degree of mal-alignment, the involvement of the soft tissues or presence of arthritis requires investigations in the form of X-rays and scans.
The diagnosis will be given to you during your outpatient appointments along with the treatment options and the likely outcomes. The treatment will depend on the cause of your injury with traumatic injuries often requiring surgery. In chronic cases conservative care is normally tried in the first instance and if this fails then an operation might be considered.
The X-ray above shows loss of alignment across the midfoot joints, irregular joint surfaces as a result of multiple fractures.
The X-ray to the left demonstrates well aligned midfoot joints with no signs of arthritis
Conservative care
Orthoses (Insoles), ankle braces
These devices help hold the foot in a neutral position and can support the arch when walking. They do not cure the problem, but they can minimise the movement across the midtarsal joints alleviating pain, although they are generally only effective in supportive shoes.
Managing pain
Anti inflammatories and analgesics
Local steroid injections
Supportive shoes
If the shoe is to provide support it needs to reduce unwanted motion. Therefore, it needs to be fairly stiff and to be held firmly to the foot with laces that are securely fastened.
Orthoses
Hoka walking shoe
Surgical Management
Surgery should only be considered if conservative care has failed, except when the deformity arises from an acute injury such as a fracture or tendon rupture. The operation depends on the underlying cause, the common operations have described below.
Arthritis of the midfoot
Investigations will enable us to confirm which joint or joints are arthritic. There are no joint replacements available for this area of the body. Given that the movement in this part of the foot is minimal, most patients fair well with fusion of the affected joints.
Joints are covered by articular cartilage which allows a bone to glide over another without symptoms. In the case of arthritis this covering is lost with the bones grinding and subsequent pain.
The prognosis following the surgery should be resolution of this arthritis pain. However, the more joints that are fused the stiffer the foot becomes with an increasing requirements on the surrounding joints to compensate, over time this can result in these joints showing wear and tear.
A car crash has resulted in extensive fractures and poor alignment of the midfoot, with the left side worse than the right. The left foot has subsequently undergone a fusion of all the midfoot articulations (eight joints), whereas the injury on the right was less extensive and just three joints were fused, with less stiffness and better function as a result.
Metatarsus adductus
Metatarsus adductus is the medial deviation of the metatarsals and often present with a bunion. In some cases, patients also develop arthritis in the midfoot with additional pain. The cause of metatarsus adductus is not fully understood with a combination of nature and nurture suspected. It can occur in isolation or as part of a more complex condition such as club foot.
Metatarsus adductus surgery normally involves realignment by fusing the medial midfoot joints. In a paper published by the department the outcomes following surgery on 59 patients were examined.
The conclusion following the investigation was that this procedure is very effective in correcting the deformity with a significant improvement in patient reported outcome measures one-year post procedure. Complications were noted with removal of the fixation in nine cases, stiffness of the big toe joint in three patients and one patient having one joint that failed to fuse, although no further treatment was required as it was not painful.
This X-ray shows a significant bunion (hallux valgus) only. The first metatarsal (a) in isolation has drifted away from the second (b)
This X-ray shows a bunion, however the metatarsus adductus angle is significant, reflecting the medial drift of the first three metatarsals towards the inside of the foot. Now the bunion cannot be corrected by just addressing the first metatarsal alone.
The far X-ray shows the bunion and metatarsus adductus angles having been successfully addressed by fusion the medial three metatarsals with screw fixation.
Lisfranc injury
This relates to fracture dislocation of the metatarsal and midfoot joints following an injury. The literature notes that up to 20% of these injuries are missed. An early and accurate diagnosis is essential in preventing malalignment and the potential for persistent pain and arthritis.
The diagnosis requires advanced imaging to determine the degree of bone, joint and ligament damage. In the past conservative care was considered the first line treatment with a below knee cast. However, this resulted in poor outcomes with most studies now suggesting either percutaneous pins or screws to manage the poor alignment whilst many now recommend an open reduction of the and internal fixation.
Studies show that the most common sequalae following a Lisfranc injury is subsequent arthritis pain in as many as 60% of cases. Depending on the pattern of injury a fusion of the medial or medial three metatarsal cuneiform joints might be required.
Preoperative Assessment
Prior to having a general anaesthetic, you would be reviewed by the nurses to ensure that you were fit and well. You will be given all the relevant information on general anaesthesia and the opportunity to ask questions.
Day surgery
These operations are normally carried out on a day care basis. You would be admitted to the hospital on the day of your operation and shown to the ward. A member of the team will confirm your consent form and mark the surgical site.
General Anaesthesia
You will be put to sleep by the anaesthetic team for the duration of your operation waking up in recovery. In addition, a local anaesthetic block in the back of your knee (Popliteal block) will be administered. This will numb your foot and lower leg providing pain relief for the 12 to 36 hours following the operation. It will also temporarily block your ability to move your foot and toes.
In adult patients the popliteal block is often performed prior to you being put to sleep. As the anatomy behind the knee varies a little from person to person, a nerve stimulator is used to accurately identify the nerves. This sends a small electric current down the needle so that when the nerve is approached it is stimulated. This means that the muscles controlled by that nerve begin to contract and relax causing the foot to ‘flick’. If you are conscious it is a strange sensation, but it helps us to deliver the anaesthetic around the nerve with precision.
Reducing the risk of a blood clot (DVT)
Being in a cast and non-weightbearing places you at an increased risk of developing a DVT, if the clot travels to the lung (pulmonary embolism) this could be fatal.
You will be shown how to inject a drug (low molecular weight heparin) using a very small needle into the fat around your tummy. This thins the blood reducing the risk of you developing a DVT.
The needle is very fine and for most patients it is not painful, it can leave a bruise, so we recommend that you move the injection sites around your tummy. These injections will need to be continued whilst you are in a cast non weightbearing.
The operation
The operation normally lasts for approximately 90 minutes with a cast put on the leg in theatre whilst you are asleep.
The cast will start from just below your knee to your toes allowing us to maintain correction whilst the body is healing, reducing the likelihood of damage. Dissolving sutures will be used to close the skin.
Recovery
You must rest with the leg elevated for the first 48hrs (essential ambulation only). It is important that you keep the cast clean and dry.
X-rays will be taken to ensure good position and stable internal fixation and at 8 and 12-weeks signs of bone healing. A Limbo cast cover can be bought to enable bathing without getting the limb wet and increasing the risk of infection.
For some patients an additional partial weight bearing cast is applied for 4 weeks. The length of time you are in a cast for depends on the procedure and how well you are healing.
Returning back to activity and regular footwear is gradual and very much depends on the type of operation, your body’s healing response and the individual’s level of motivation.
Full recovery takes 7-12 months.
Possible complications
Approximately 700 patients undergo foot surgery annually within the Department of Podiatric Surgery at West Middlesex University Hospital.
Most patients have an uneventful recovery. Outlined below are the common problems or those rare complications with serious outcomes. In cases where we don’t have accurate audit, we have used published results from the podiatric literature. These are accompanied by an asterisk *
Prolonged swelling taking more than 6 months to resolve occurs 1 in every 500 operations*
Haematoma – a painful accumulation of blood within the operation site. No recorded incidents.
Thick and or sensitive scar – no audit data is available.
Screws and plates were removed from 118 patients during a twelve-month period. This is often planned but can occur as a result of irritation.
Adverse reaction to the post-operative pain killers. 1 in every 50 patients report that the codeine preparations can make them feel sick.*
Infection of soft tissue. The incidence is 1 in every 83 operations*
Infection of bone occurred in 3 out of 916 patients.
Delayed healing of soft tissue or bone. No audit data is available.
Circulatory impairment with tissue loss occurred in 3 out of 9000 patients over a 10 year period.
Loss of sensation can occur although this is usually transient but can take up to a year to resolve.
Deep vein thrombosis which can result in a clot in the lung is potentially a life-threatening condition. Within the published literature, the overall incidence of VTE is thought to be 0.9% in foot and ankle surgery.
Chronic pain syndrome: this is where the nervous system dealing with pain over reacts in a prolonged manner often to a minor incident. This normally requires management by specialists in this condition and doesn’t always resolve. This is a rare complication with no audit data available.
Reoccurrence of the deformity or failure of the operation
Development of secondary problems including overloading of joints adjacent to the ones operated
The risk of having a complication can be minimised when the patient and all those concerned with the operation and aftercare work together. This starts with the pre-operative screening and continues through to the rehabilitation exercises.
Pre-operative screening of your health allows us to determine whether you are fit for surgery. It is important that you disclose your full medical history. If there is a query regarding your health, then further investigations or the advice of other surgical and medical specialties will be sought.
The surgeon and the theatre team will ensure that the operation is performed effectively and with the minimum of trauma.
You can improve the healing process and reduce the risks of complications by:
Adhering to the post-operative instructions which include resting and elevating the operated leg. Keeping the wound clean and dry until advised otherwise is essential. Please ask the team if you are not sure what to do.
Having a healthy diet is important. This provides the nutrition required for healing.
Smoking is associated with a 20% increased risk of delayed or non-healing of bones.
Alcohol can interact with the drugs that we will prescribe and in excess can impair wound healing.
Post-operative exercises and in certain cases physiotherapy will be advised. This helps improve the flexibility, strength and stability of your foot.
Podiatric surgeons evaluate, diagnose, prevent and treat diseases, disorders and conditions affecting the foot and all associated structures. This is carried out in keeping with the individual’s education, training and experience, in accordance with the ethics of the profession and applicable law.
Podiatric surgeons are not medical doctors.
Podiatric Surgical Training
3 year: Degree in Podiatry (BSc)
2 year: Masters in the theory of podiatric surgery (MSc)
2 year: Surgical training programme (Podiatric Surgical Trainee) Final fellowship examinations (Podiatric Surgeon)
3 year: Specialist training (Podiatric Registrar)
Accreditation with the Faculty of Podiatric Surgery